


Transient vision loss (TVL) refers to a complete or partial temporary blurring or blacking out of the vision, lasting less than 24 hours, in one or both eyes.1 Patients may note that it feels like a curtain or veil coming down over their sight or a sudden darkening of vision.
TVL is a complaint that should raise a large red flag and warrants specific follow-up questions to determine the workup needed to identify the underlying cause, be it neurologic, compressive, vascular, or ophthalmic.
Determining the cause of transient vision loss
There are several important questions to ask when determining the cause of transient vision loss.
They include:
- Was the vision loss monocular or binocular?
- Is there any pattern with when it occurs? This could include postural changes, after looking at their cell phone while lying in bed, after exercise or exposure to heat, or if it occurs only in specific directions of gaze.
- Are there any systemic health risk factors present? This is especially relevant for the vascular causes of transient monocular vision loss. You should also inquire whether the patient has a history of stroke.
- What is the duration of the transient vision loss? Distinguishing between seconds, a few minutes, up to 20 to 30 minutes, or longer can assist in diagnosis.
- Has the patient experienced any other associated symptoms? Any giant cell arteritis (GCA) symptoms (i.e., jaw claudication, temporal tenderness, fatigue)? Eye pain? Headaches?
Patients with vascular risk factors, including cardiovascular disease, history of stroke, diabetes, hypertension, elevated cholesterol, advancing age, and tobacco use, are the main demographic of concern.
Download the Transient Vision Loss Protocol Cheat Sheet
📝
Transient Vision Loss Protocol Cheat Sheet
This cheat sheet describes the various potential causes of transient vision, and provides guidiance for ordering imaging, managing symptoms, and referring patients.
Vascular causes of transient monocular vision loss
There are a range of vascular causes tied to transient monocular vision loss (TMVL), including ischemic optic neuropathy and transient retinal arterial occlusion.
Ischemic optic neuropathy
Giant cell arteritis should always be considered in all patients over age 50 with TVL. New onset temporal or occipital headaches are present in 90% of cases.2 Inquire about fatigue, scalp tenderness, jaw and tongue claudication (e.g., do they get tired while eating/chewing?), fever, and weight loss. Episodes of TVL are present in 32% of GCA patients and typically start 8.5 days before permanent vision loss.3
With any suspicion of TVL from GCA, same-day referral for lab work is crucial. Labs for GCA workup are erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and complete blood count (CBC) with differential. If the patient’s blood work is abnormal, starting treatment with high-dose intravenous (IV) steroids and performing a temporal artery biopsy is warranted.
These labs should be ordered in all patients with transient monocular vision loss, even in patients who have no other symptoms of temporal arteritis. Up to 20% of patients with temporal arteritis and ocular symptoms have otherwise occult disease.4
Transient retinal arterial occlusion
TVL from this condition is usually due to cholesterol, platelet-fibrin, or calcific emboli causing a temporary blockage of retinal circulation. These emboli can break off from atherosclerotic carotid arteries or are caused due to valvular heart disease.5
The painless blockages cause TVL, known as amaurosis fugax, and are usually experienced as a temporary darkening of vision. If the emboli are too large to continue traveling downstream in the retinal arteries, they can also cause more permanent vision loss through a branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO).6
Due to the temporary retinal ischemia caused by the plaque or emboli, patients who have their vision return after TVL may notice a new visual field defect. These are most commonly located nasally as the emboli get stuck in the small temporal arteries.7 In one study, amaurosis fugax was present in 14.20% of patients with branch retinal artery occlusion and in 12.18% of patients with central retinal artery occlusion.8 It has an incidence of 14/100,000 people per year.9
The vision loss may last up to 30 minutes, but in most cases, it resolves after a few seconds to a few minutes. According to studies, patients with transient monocular vision loss associated with carotid artery atherosclerosis have a 2% risk of stroke over the next year.10
Those with severe stenosis, have a 16% chance of suffering an ipsilateral stroke over the next 3 years.11 To decrease the likelihood of subsequent ischemic events, it is imperative that diagnosis and treatment focus on secondary prevention measures.
The importance of referral with transient retinal ischemic attack
Any patient with a retinal transient ischemic attack should be referred for immediate workup at a stroke center.12
This workup includes:
- Brain magnetic resonance imaging (MRI) with contrast
- Electrocardiogram
- Echocardiogram
- Vascular imaging with computed tomographic angiogram (CTA) or magnetic resonance angiography (MRA) of the head and neck
Of note, brain infarction is demonstrated on MRI in 25% of patients with acute retinal ischemia and in 18% of patients with a retinal transient ischemic attack.13,14
Figures 1 and 2 demonstrate fundus photography of retinal emboli in the inferior temporal arcade.

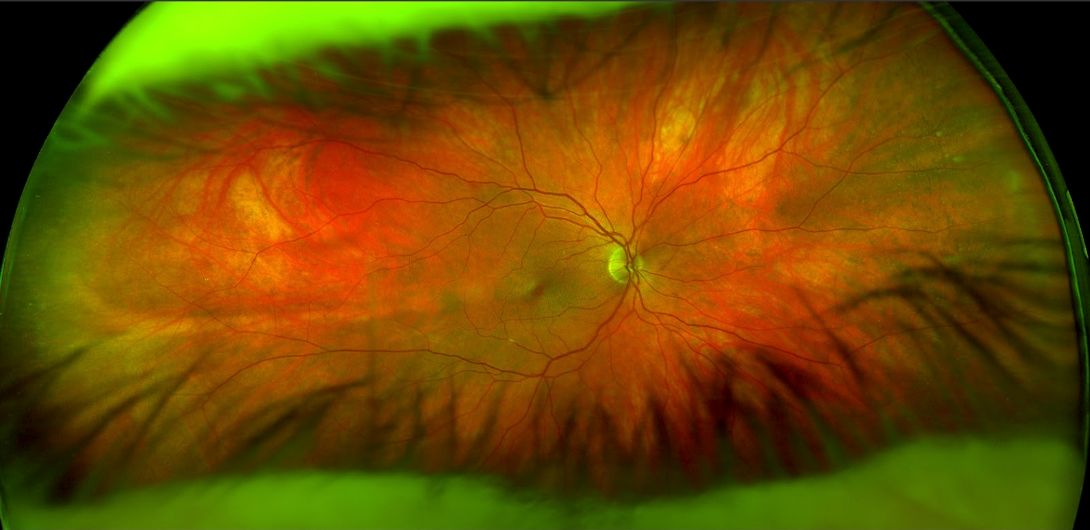
Figure 1: Courtesy of Kristin McArdle, OD.

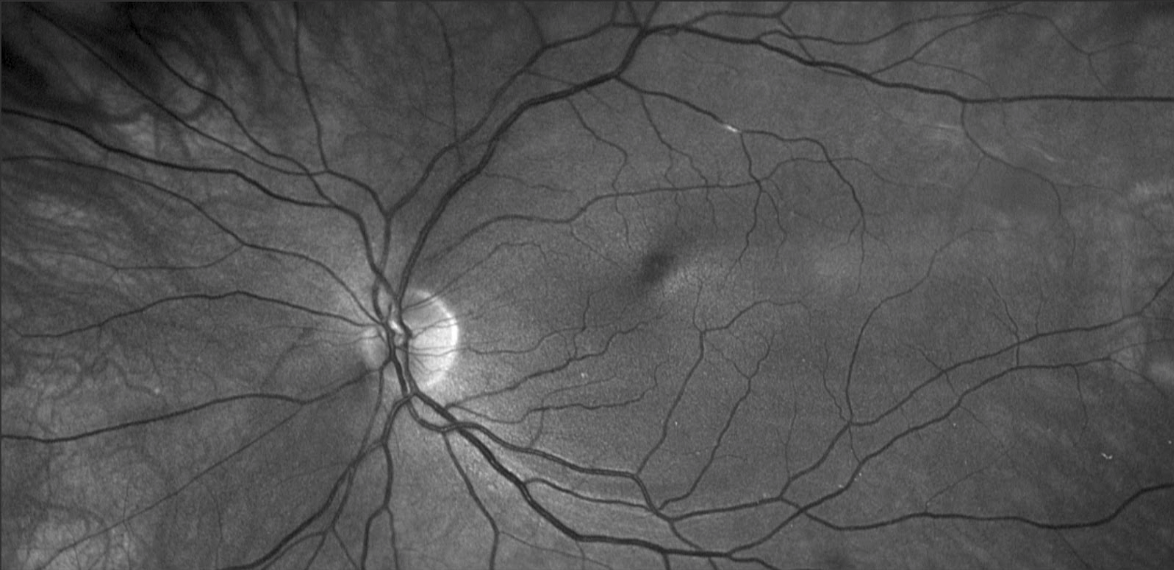
Figure 2: Courtesy of Kristin McArdle, OD.
Transient or impending central retinal vein occlusion
TVL with CRVO is usually described as blurry or cloudy vision rather than a blacking out of vision. There have been case reports of TVL lasting 20 minutes to 4 hours related to impending or transient CRVO.
This is much longer than the typical 3-minute blacking out of vision typical in an arterial occlusion.15 A study documented episodes of TVL in 4.86% of those with CRVO and in 0.35% with BRVO.16
If the TVL is occurring in younger patients, bloodwork to assess for clotting disorders should be ordered. For patients 50 and older, a workup for cardiovascular risk factors should be completed urgently.
Ocular ischemic syndrome
The most common demographic for ocular ischemic syndrome (OIS) is men over age 50, likely due to the higher incidence of atherosclerotic and carotid artery disease in these patients.17 TVL from OIS occurs when blood flow to the eye is obstructed due to a temporary embolus blocking the central retinal artery or one of its branches.
With an estimated incidence of 7.5 cases per million persons per year, OIS is a relatively rare, though potentially underdiagnosed condition.18 A history of TVL is present in about 10 to 15% of patients with OIS. The TVL will present as a dark or black shade across the vision that lasts for a few seconds to minutes.19
Pain due to increased intraocular pressure (IOP) or ischemia may be present in up to 40% of the eyes with OIS.20 Ischemic pain sets in gradually over hours to days and may worsen when the patient is upright. The pain is commonly described as a dull ache in the affected eye, temple, and forehead.
Underlying conditions that can cause OIS
Generally, ≥90% stenosis of the ipsilateral carotid artery is present in eyes with OIS. Patients with OIS have systemic vascular co-morbidities related to atherosclerosis. These include a history of cerebrovascular accident or transient ischemic attack, ischemic heart disease, diabetes, peripheral vascular disease, and systemic hypertension.
These patients also have an increased risk of stroke at 4% per year.21 OIS can present with a wide variety of ocular signs, including mid-peripheral retinal hemorrhages, neovascularization of any type, and inflammation in the form of iris synchiae and iridocylitis.22
Due to the systemic nature and extensive ocular complications of OIS, treatment is multifactorial. Ocular management targets anterior segment inflammation, neovascular glaucoma, and elevated IOP. A carotid ultrasound or Doppler ultrasound is needed to determine the extent of carotid artery blockage.
If the blockage is greater than 50 to 60%, usually a carotid endarterectomy will be performed.23 Coordination with the patient’s primary care physician (PCP) and cardiologist is vital to prevent future heart attack and stroke.
Check out the downloadable cheat sheet on transient vision loss protocols!
Compressive causes of TMVL
Orbital mass
Compression of the optic nerve can cause transient vision loss with changes in gaze or eye movements, called gaze-evoked amaurosis. Optic nerve or orbital tumors are rare causes of transient monocular vision loss.
Patients with these tumors may be symptomatic for positive visual phenomena, including flashes and scintillating scotomas. The vision loss only lasts for seconds and baseline vision returns on straight-ahead gaze.24
The compression of the optic nerve and vascular supply causes transient ischemia and is likely the mechanism causing the TVL from a mass. Gaze-evoked amaurosis is a red flag for a tumor compressing on the optic nerve and warrants urgent MRI imaging and neuro-ophthalmology or neuro-surgery referral.25
Thyroid eye disease
Thyroid eye disease (TED) has been known to cause transient visual obscuration lasting 3 weeks to 2 months.26 While this does not fit into the criteria of lasting less than 24 hours in duration, it may be worth keeping as a differential diagnosis. Ocular surface disease (OSD) due to eyelid retraction can also cause transiently blurred vision in TED patients.27
Engorgement of the extraocular muscles can cause compression of the optic nerve resulting in vision loss. Management of the underlying disease with medications or surgical procedures to decompress the optic nerve is necessary.
Ocular causes of TMVL
Ocular surface disease
Tear film abnormalities resulting from dry eye syndrome, contact lens wear, epiphora, or blepharitis are common causes of transient visual disturbance. These conditions should be differentiated from true TVL since the patient will experience fluctuating blurring vision that will vary with blinking or the use of lubricating drops rather than a blacking out of vision.
The duration of blur may be variable, from several minutes to several hours. In particular, patients using contact lenses and older patients with a history of neurodegenerative disorders such as Parkinson’s disease may experience a foreign body sensation and conjunctival injection with transient visual disturbance.24
Ophthalmic evaluation with a slit lamp may show inflammation and debris along the lid margins, abnormal tear film breakup time, and superficial punctate keratitis. Management of the OSD should allow the tear film to stabilize and decrease the frequency of blurry vision.
Transient smartphone blindness
Transient smartphone blindness (TSB) is a recent phenomenon associated with smartphone use while lying supine in the dark. While lying on their side on a bed or sofa, the patient’s upper eye looking at the screen is light-adapted while the lower eye being occluded (by a pillow or sheets) is dark-adapted.
After turning off the phone, the patient may realize they cannot see in the dark with the eye that had been looking at the bright screen. Vision returns within minutes as the eye dark adapts.28 Taking a thorough history is important to differentiate TSB from other causes of painless TVL such as amaurosis fugax.
Intermittent angle closure
During angle closure, patients can experience eye pain, frontal headache, blurred vision, and nausea. In an acute angle closure attack, clinical signs include elevated IOP, corneal edema, and mid-dilated, poorly reactive pupil.
Intermittent angle closure is more difficult to diagnose as the symptoms are more mild and non-specific. Patients may be asymptomatic or may have similar symptoms as acute angle closure but will only experience them transiently. Risk factors for angle closure include female gender, hyperopia, and a shallow peripheral anterior chamber.29
Acute angle closure is an ocular emergency due to the optic nerve damage that can rapidly occur if IOP remains elevated for hours or days.30 Treatment for both intermittent and acute angle closure includes lowering IOP followed by laser peripheral iridotomy or early crystalline lens extraction. It is critical that these patients are identified to prevent irreversible glaucomatous vision loss.
Pigment dispersion syndrome
Pigment dispersion syndrome (PDS) is most commonly diagnosed in myopic males in their 30s, but can also occur in women and in different age groups.31 Patients may present with halos or transiently blurred vision due to episodes of increased IOP. These events can be brought on by exercise or dim lighting conditions.
Diagnosis of PDS is made when the following findings are present:
- Mid-peripheral iris transillumination defects (TIDs)
- Heavily pigmented trabecular meshwork
- Pigment on the cornea endothelium (Krukenburg spindles)
The treatment of PDS revolves around IOP control with topical medications or surgical intervention and requires routine monitoring similar to cases of primary open-angle glaucoma (POAG). Some studies have shown that PDS patients are more likely to require surgery than their POAG control counterparts.32
Uveitis-glaucoma-hyphema syndrome
Uveitis-glaucoma-hyphema (UGH) syndrome is an uncommon cause of transient monocular vision loss but is one that can occur after cataract removal and intraocular lens (IOL) implantation. TVL from this condition presents as a blur or fogginess that occurs rapidly over minutes and then takes several hours to resolve.
UGH syndrome occurs when the haptics from the IOL are causing inflammation in the ciliary sulcus, such as in a posterior capsule IOL, or are abrading the iris as in an anterior chamber IOL. Misdiagnosis of this condition as amaurosis fugax can cause the patient to be treated with a blood thinner, which could increase the likelihood of a hyphema rebleed.33
Treatment is needed if TVL recurs regularly or glaucoma develops. Adjustment or replacement of the IOL allows for complete resolution but is reserved for severe cases due to potential complications. In milder cases, uveitis can be controlled with topical corticosteroids, glaucoma can be treated with topical IOP-lowering medication, and any identifiable iris blood vessels causing bleeding can be cauterized with a laser.34
Uhthoff’s phenomenon associated with demyelinating optic neuritis
A history of optic neuritis with multiple sclerosis (MS) or neuromyelitis optica (NMO) is related to Uhthoff’s phenomenon, which can cause blurred vision or color desaturation after increased body temperature.
This can be brought on by exercise, a hot shower, or hot external temperatures.35 Diplopia, nystagmus, and pain on eye movement can also present in cases of acute optic neuritis. MS is most common in women ages 20 to 40 living further from the equator.36
NMO is typically diagnosed in females aged 30 to 50 and is more common in those of African or Eastern Asian descent than those who are white.37 Blurred vision from Uhtoff’s phenomenon will resolve within an hour and under circumstances where the heat sources are removed, or active cooling measures are applied. Simple strategies such as taking cold showers, application of ice packs, and cold beverages can be effective.38
After an episode of acute optic neuritis, blurred vision and color vision can take months to return to normal. After an acute episode, a majority of patients will achieve 20/20 vision within 1 year while 8% of patients retain a visual acuity worse than 20/40.
However, recurrent episodes are associated with less favorable vision outcomes.39 Based on the results of the Optic Neuritis Treatment Trial study, the treatment of acute optic neuritis may include IV methylprednisolone followed by oral steroid taper.40
The treatment for NMO is similar but requires longer and more intense steroid treatment. This treatment speeds up recovery time but does not improve long-term outcomes. Management with immunosuppressive therapy for the underlying condition is also needed to prevent future episodes of optic neuritis.
TVL caused by vitreous abnormalities
Vitreous floaters or vitreous hemorrhage can cause transient blurred vision lasting for a few seconds at a time. The sensation can be described as a filminess, a spot, or a sheet of blurriness coming over the vision in the case of vitreous syneresis or a large central floater. The severity of the vitreous hemorrhage determines the level to which the vision is affected.
Morning time upon waking tends to be when these patients are most symptomatic. This is likely due to the patient lying flat while sleeping and having the floaters or blood settle more centrally in the vitreous. As the day goes on, gravity will take effect and move the opacities inferiorly.
In the case of vitreous hemorrhage, the underlying cause must be determined, and depending on the severity of vision loss, a B-scan to rule out retinal detachment may be necessary. For long-standing large central floaters, a floaterectomy or vitrectomy with a retinal specialist can be considered for symptomatic patients as an elective procedure.24
Carotid artery dissection
Another rare cause of transient vision loss is dissection of the internal carotid artery. One study reported that 28% of patients with carotid artery dissection experience TVL, often in conjunction with painful Horner’s syndrome on the same side.41
Symptoms of TVL can occur due to compromised blood flow to the eye and brain. Other symptoms of carotid artery dissection include headache, scalp pain, neck pain, and one-sided weakness. This is considered a medical emergency and requires immediate referral to the hospital for treatment and stroke prevention.24
Busy now? Download the Transient Vision Loss Protocol Cheat Sheet to review later!
Causes of transient binocular vision loss (TBVL)
It can be difficult for patients to determine if their episode of transient vision loss was monocular or binocular. Some findings that can help guide the diagnosis include the patient being unable to read during the episode, vision loss to one side, and positive visual phenomena described, such as zig-zags or scintillating scotomas.
Vascular causes of TBVL
Vertebrobasilar insufficiency
This is a type of transient ischemic attack (TIA) that occurs when there is insufficient blood flow to the brain via the vertebral and basilar arteries, usually caused by atherosclerotic plaque. The arteries that feed the occipital lobe and other areas of the brain are affected.
Vertebrobasilar insufficiency (VBI) occurs due to a drop in blood pressure and can cause a TIA. The transient vision loss may be isolated or associated with other neurological symptoms like vertigo, diplopia, headaches, dysphagia, and unilateral or bilateral weakness.42
Of note, 25% of strokes and transient ischemic attacks are in the vertebrobasilar distribution. Due to the higher occurrence of cardiovascular risk factors in the male population, these are more common in men in their 70s and 80s.43
Management of this condition is typically focused on limiting activities that cause drops in blood pressure, like quick position changes, dehydration, or exertion. A workup for ischemic stroke must also be done urgently.
Ocular causes of transient binocular vision loss
Abnormal optic discs
TVL from abnormal optic discs can be caused by papilledema or by optic nerve head drusen.44 Typically, the condition is bilateral but patients often note the vision changes asymmetrically between the two eyes.
These episodes of transient vision loss can be brought on by postural changes or valsalva maneuver, last for seconds at a time, and can be described as a gray-, black-, or white-out of vision.24 Transient visual obscurations are commonly associated with papilledema from elevated intracranial pressure.
Papilledema should be differentiated from optic disc drusen, and a workup ordered to determine the underlying cause of the disc edema. TVL is also present in 10% of patients with optic nerve drusen and can present monocularly or binocularly.45
If the cause is determined to be optic disc drusen, there is no strong evidence to support treatment for those without visual field defects. Periodic monitoring for potential sequelae, such as peripapillary choroidal neovascularization, is warranted.
Figures 3 and 4 demonstrate fundus photography of papilledema with peripapillary hemorrhages.


Figure 3: Courtesy of Kristin McArdle, OD.


Figure 4: Courtesy of Kristin McArdle, OD.
Accommodative spasm
Spasms of the accommodative system can cause blurred vision at far and near. Typically this is most noticeable to patients when switching from distance to near or vice versa. It can worsen with prolonged near work.
This is most common in children, but early presbyopes may also complain of similar symptoms. These symptoms can be managed with bifocal lenses or vision therapy for children.46
Fluctuating blood glucose
Patients with uncontrolled diabetes mellitus may experience transient visual disturbance due to osmotic changes in the crystalline lens. These changes thicken the lens and cause a myopic shift in refraction. The blurry vision may last from several minutes to several hours, depending on blood sugar levels and fluctuations.47
On examination, visual acuity may improve on pinhole testing or subjective refraction. Gaining stability of the blood sugar with medication and lifestyle modification is crucial. Co-management with the patient’s endocrinologist or PCP is also necessary to prevent further ocular complications from diabetes.
Neurologic causes of TBVL
Migraine with aura
The International Headache Society diagnostic criteria for a retinal or ocular migraine require at least two attacks of fully reversible monocular positive visual phenomena such as flashing lights, zigzag lines, or scintillating scotoma—before or during the episode of vision loss associated with a migraine headache.48
The TVL typically lasts 5 to 30 minutes and may recur several times during the day.49 According to the American Migraine Foundation, about 20 to 30% of migraine sufferers have the aura symptom with their headaches.
Co-management with neurology and avoidance of migrainous triggers can help to decrease the incidence of migraine with aura. This is considered a diagnosis of exclusion, and these patients still need a thorough workup to rule out other causes of TVL.
Occipital seizures/occipital lobe epilepsy
Binocular vision loss can occur with occipital seizures. The duration of vision loss during the seizure varies between less than 1 minute and days or can be permanent. This condition can occur in both adults and children and is related to a diagnosis of epilepsy.50
These episodes of vision loss are characterized by positive visual phenomena, such as bright-colored or dark rings and spots or shapes that are constant or flashing. More complex visual hallucinations can also occur and often include scenes related to past experiences. An electroencephalogram (EEG) is needed for diagnosis, and these patients typically respond well to anti-epileptic drugs under the care of neurology.
Conclusion
There are many causes of transient vision loss. The first step towards a correct diagnosis is obtaining a thorough case history. A complete ophthalmic examination will also help to determine if the cause is ocular, neurologic, compressive, or vascular.
Additional imaging and testing should be ordered based on the differential diagnoses, with immediate workup for GCA and ischemic vascular causes if the findings are suggestive.
Determining if there are any precipitating events, such as eye pain after exercise or with bedtime smartphone use can align with diagnoses that would prevent unnecessary treatments and costs to the patient.
Avoiding irreversible vision loss and potentially saving the patient’s life is of utmost importance in cases of transient vision loss. As today’s primary eyecare providers, optometrists must be ready to diagnose and manage their patients with TVL promptly and appropriately.


